Heart
Lab Summary
This lab explores the relationships of the heart to surrounding structure and their clinical importance. Cardiac surfaces, the interior structure of the heart and coronary circulation is taught. The interior of the heart is taught through in situ and isolated dissections.
Lab Objectives
- Describe the chambers of the heart that contribute to the cardiac surfaces and borders.
- Describe the pericardium.
- Explain the significance of the transverse pericardial sinus.
- Describe the location of the major branches of the coronary arteries in relation to the atrioventricular and interventricular grooves.
- Describe the position and significance of the ligamentum arteriosum and fossa ovalis.
- Name the valves of the heart and the chambers / vessels they connect.
- Describe the approximate location of the sinoatrial (SA) and atrioventricular (AV) nodes.
- Describe the conduction system of the heart.
- Describe the functional importance of papillary muscles and chordae tendineae.
Lecture List
The Heart, Exposure of the Heart, Coronary Vessels, Removal of the Heart, Bisecting the Heart, In Situ Dissection of the Heart
Anatomy of the Heart
The Heart Gallery
 1.1a) Ribs show us where to listen for the valves
1.1a) Ribs show us where to listen for the valves
















Exposure of Heart
Pericardium
Incise the pericardium in the anterior midline. Open further with transverse incisions at the apex and base.
Identify the fibrous pericardium and the parietal and visceral (epicardium) layers of the serous pericardium.
 2.1a) Pericardial incisions
2.1a) Pericardial incisions


Cardiac Surfaces
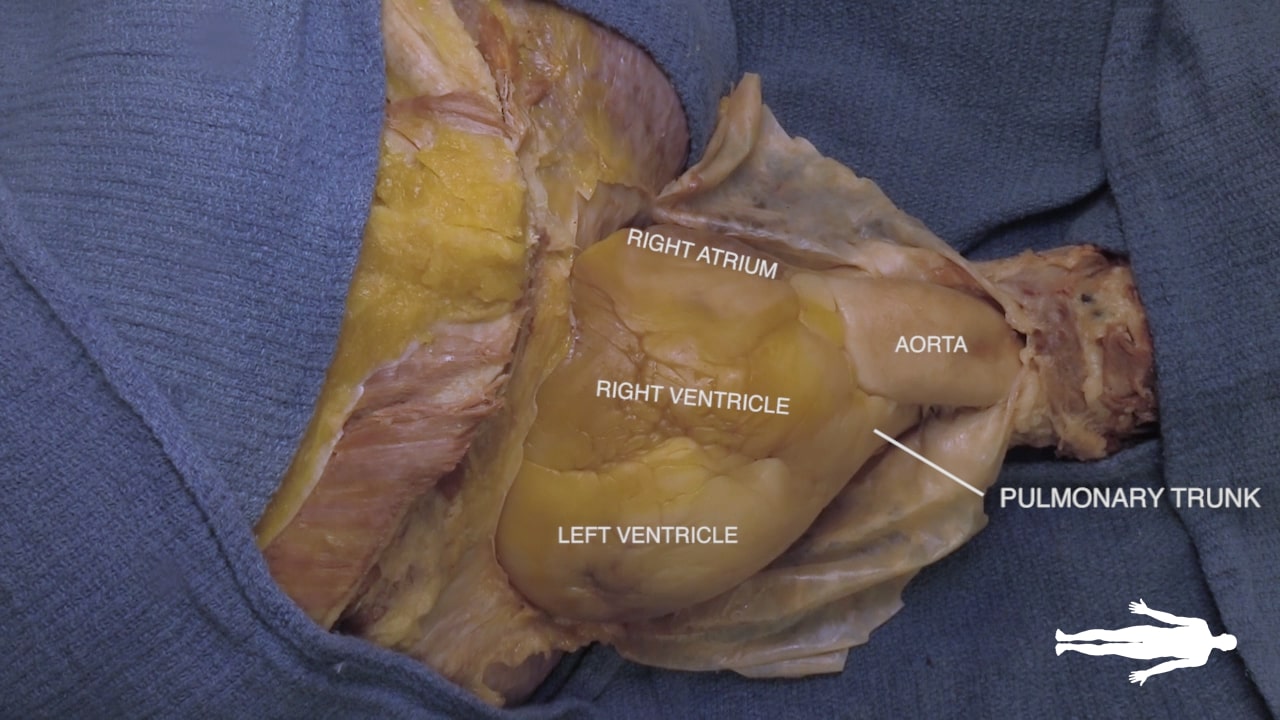
Identify the chambers of the heart, aorta, pulmonary trunk, superior and inferior vena cavae and pulmonary veins.
Lift the heart to view its diaphragmatic surface.
 2.2a) Anterior heart
2.2a) Anterior heart


Transverse Pericardial Sinus
Place an instrument posterior to the pulmonary trunk and ascending aorta. Note that cardiac output is anterior to the probe and the venous inflow is posterior. This space is the transverse pericardial sinus and an important landmark in cardiac surgery.
 2.3a) Transverse pericardial sinus
2.3a) Transverse pericardial sinus

Left Cardiac Surface
On the left side of the heart, locate vagus nerve (X), ligamentum arteriosum and left recurrent laryngeal nerve.
The vagus nerve lies along the aortic arch. The ligamentum arteriosum connects the left pulmonary artery and the arch of the aorta. The left recurrent laryngeal artery can be identified branching from the vagus nerve and passing posterior to the ligamentum arteriosum.

Right Cardiac Surface
On the right side of the heart, re-identify the hilus of the lung and find the arch of the azygos vein passing superior to the hilus of the lung to enter the superior vena cava.
Identify the atrioventricular groove on the right side of the heart. The right coronary artery lies in this groove.

Coronary Vessels
Diagram of Coronary Vessels

Coronary Vessels
 3.2a) Right coronary artery
3.2a) Right coronary artery


Left Coronary Artery
 3.3a) Anterior interventricular artery (LAD)
3.3a) Anterior interventricular artery (LAD)

Removal of Heart
Removing the Heart
 4.1a) Division of the aorta
4.1a) Division of the aorta



Bisecting the Heart
Bisecting the Heart
 5.1a) Coronary sinus
5.1a) Coronary sinus

Cardiac Structures
 5.2a) Four chamber view
5.2a) Four chamber view





In Situ Dissection
Complex in situ Dissection
 6.1a) Anterior heart
6.1a) Anterior heart







{kind=link}
Cardiac Electrical System
Physical Examination of Heart
Cardiac Clinical Correlations
Trauma: Cardiac box: The “cardiac box” is the region demarcated by the sternal notch (superiorly), xiphoid process (inferior), and midclavicular lines (laterally). Penetrating trauma or blunt force to the cardiac box can injure the heart. The right ventricle, being the most anterior structure of the heart, is most prone to penetrating injury. A life-threatening consequence of cardiac trauma is cardiac tamponade where blood accumulates within the pericardial sac and compresses the heart. For more information of thoracic trauma, review the “deadly dozen”.
Procedure: Atrial fibrillation, the left atrial appendage, and TEE: Atrial fibrillation (Afib) impairs the contraction and emptying of the atria which allows blood to pool and clot. These clots generally form in the left atrial appendage (LAA), a pouch-like portion of the left atrium. Return to sinus rhythm can dislodge clots into the aorta (causing stroke) therefore high-risk patients should undergo work-up for LAA thrombus prior to cardioversion. Because its far posterior location and interference from the bones of the spine/rib cage, the left atrium cannot be reliably viewed through transthoracic echo (external ultrasound probe placed on external chest). Importantly, the esophagus is located immediately posterior to the left atrium, Therefore, the gold-standard for diagnosing LAA thrombus is transesophageal echo (TEE) which entails passage of an ultrasound probe through the mouth and into the esophagus of an anesthetized patient.
Embryology: Foramen ovale and ductus arteriosus: In utero, lungs are fluid-filled (i.e. high-pressure system) therefore most blood pumped by the right heart bypasses the lungs through two structures:
- the ductus arteriosus: allows blood to move from pulmonary artery to aorta
- the foramen ovale: allows blood to move from the right atrium to the left atrium
At birth, the lungs become a low-pressure system prompting signaling events that precipitate closure of these structures to leave remnants:
- ductus arteriosus becomes the ligamentum arteriosum
- fossa ovalis becomes the foramen ovale
If these structures remain inappropriately open (i.e. patent), inappropriate shunting of blood may occur. A patent ductus arteriosus (PDA) allows blood to move from the higher-pressure aorta to the lower pressure pulmonary trunk, pathologically increasing blood flow across the heart and lungs. A patent foramen ovale (PFO), while usually asymptomatic, is associated with intermittent right to left shunting when RA pressure rises (see paradoxical emboli for more information).
Surgery/Autopsy: Cardiac surgery and phrenic nerve: Within the thorax, the right and left phrenic nerves pass between the fibrous pericardium and the mediastinal parietal pleura. As a result, cardiac surgeries that involve manipulation of the pericardium carry a risk of phrenic nerve injury. Clinical presentations include hiccups and difficulty breathing. Imaging may show diaphragmatic dysfunction, paralysis, or paradoxical movements.
Anatomical Variations: Coronary “dominance”: The posterior descending artery (PDA) feeds the posterior third of the interventricular septum. The PDA arise from the right coronary artery (70%; “right-dominance”), left coronary artery (10%; “left-dominance”), or both (20%; “co-dominance”). Knowing a patient’s cardiac dominance is critical for appropriate endovascular navigation to alleviate PDA stenosis or appropriate installation of vascular grafts during bypass surgery.
Imaging: Chest Xray is the first modality often used to image the chest, as it is fast, safe and inexpensive. However, although good for looking at large lung findings and assessing the size of the heart or placement of support devices, it does not allow for visualization of discrete cardiac anatomy. Instead, CT with contrast can be use. Echocardiogram (ultrasound) is one of the best and most common ways to evaluate the cardiac chambers and function. Cardiac MRI can be used for specialized applications to evaluate the myometrium and cardiac function, but requires much more time and is only performed at subspecialty centers.
Imaging correlate: Head to Table 13 to see a pacemaker or Table 26 to see a pacemaker, cardiac valve replacement (can you figure out which one?) and other support devices. What anatomic structures are these support devices located in? Challenge: How are the cardiac pacemaker leads placed via an endovascular approach…how did they get there??
Images (Click to Enlarge)


Autopsy images showing knife wound to heart (L) and laceration from fractured ribs (R)

TEE showing thrombus (arrow) in LAA

Autopsy image showing PFO; probe passing from RA side to LA side through opening

Fetal cardiac physiology

Autopsy image showing acceleration-deceleration aortic laceration; notice site of tear is the aortic isthmus (just distal to subclavian take-oT)

Autopsy images showing cardiac tamponade
Cardiac Video Transcript
Anatomy of the Heart: A Comprehensive Guide
This guide provides an overview of the anatomy of the heart, covering its external surfaces, internal chambers, blood supply, valve function, and conduction system.
- Anterior View and Surface Anatomy
See Complete Heart.
- Anterior Surface: Primarily formed by the right ventricle (1). Located deep to the sternum and anterior ribs.
- Right Border: Formed by the right atrium (16).
- Left Border: Formed by the left ventricle (4).
Clinical Note: Understanding these borders is essential for examining chest X-rays. Changes in the position or visibility of these borders can be diagnostically significant.
2. Posterior Inferior View
See Complete Heart.
- Posterior Surface: The left atrium (12) is situated posteriorly, resting against the vertebral column and the esophagus.
- Diaphragmatic Surface: The right and left ventricles sit on the diaphragm, forming the diaphragmatic surface of the heart.
3. Superior View of the Valves
See Valve Plane.
When the pulmonary trunk, aorta, and atria are removed, the position of the heart valves is revealed. Due to embryologic development, the valves are located close together.
- Anterior Valves: The aortic and pulmonary semilunar valves.
- Posterior Valves: The atrioventricular (AV) valves.
- Tricuspid Valve: Located on the right.
- Bicuspid (Mitral) Valve: Located on the left.
4. Arterial Blood Supply (Coronary Arteries)
The coronary arteries arise from the proximal aorta and run within the atrioventricular and interventricular grooves. See Complete Heart.
- Right Coronary Artery (19): Runs in the right atrioventricular groove and terminates posteriorly as the posterior interventricular artery (20).
- Left Coronary Artery (7): Divides into two main branches:
- Circumflex branch (11): Runs in the left atrioventricular groove.
- Anterior interventricular branch (8): Also known as the Left Anterior Descending (LAD), it runs in the anterior interventricular groove and serves as the primary blood supply for the left ventricle.
5. Venous Return and the Right Atrium
Cardiac blood returns to the right atrium via the coronary sinus, which is visible from a posterior-inferior view. See Dissected Heart.
Interior of the Right Atrium:
- Venous Openings: The Superior Vena Cava (SVC; ***) enters superiorly, and the Inferior Vena Cava (IVC; ***) enters inferiorly. The coronary sinus (2) opens adjacent to the IVC.
- Atrial Wall: The interior consists of a smooth part (derived from embryonic veins) and a rough part (representing the primitive heart). The junction between these two parts is called the crista terminalis (3).
- Fossa Ovalis: A small depression on the interatrial septum. This is a remnant of the fetal foramen ovale (***), which allowed placental blood to bypass the lungs and move from the right heart to the left heart.
- Tricuspid Valve (4): The right atrioventricular valve connecting the right atrium to the right ventricle.
6. Interior of the Right Ventricle
See Dissected Heart.
- Tricuspid Valve Attachment: The valve cusps are connected to papillary muscles (7) by fibrous cords called chordae tendineae (6) (commonly known as “heartstrings”).
- Function: The papillary muscles contract to keep the valve closed during ventricular contraction, preventing backflow.
- Outflow Tract: The smooth upper portion of the right ventricle is the infundibulum, which leads to the pulmonary valve and the pulmonary trunk (15) on the way to the lungs.
7. Interior of the Left Ventricle
See Dissected Heart.
- Ventricular Walls: The left ventricle is characterized by very thick muscular walls.
- Mitral Valve (14): Connects the left atrium and left ventricle, supported by its own papillary muscles and chordae tendineae.
- Aortic Valve (13): Located superiorly, this valve leads to the aorta and the systemic circulation.
8. Heart Valve Function and Sounds
The state of the valves changes depending on whether the heart is in systole or diastole.
Systole (Ventricular Contraction):
- The aortic and pulmonary valves are open to allow blood flow to the lungs and body.
- The atrioventricular (tricuspid and mitral) valves are closed.
- Heart Sound: The closure of the AV valves produces the S1 heart sound.
Diastole (Ventricular Filling):
- The atrioventricular valves are open.
- The pulmonary and aortic valves are closed by back pressure.
- Heart Sound: The closure of the semilunar valves produces the S2 heart sound.
Clinical Note: There are specific locations on the chest that are used to listen to the heart with a stethoscope (auscultation points)
- Aortic: Right upper sternal border, 2nd intercostal space
- Pulmonic: Left upper sternal border, 2nd intercostal space
- Tricuspid: Left lower sternal border, 5th intercostal space
- Mitral: Left midclavicular border, 5th intercostal space
- Erb’s point: left sternal border, 3rd intercostal space; location where S1/S2 are best heard
9. Cardiac Conduction System
The heartbeat is regulated by a specialized electrical system.
Right and Left Bundles: The path divides into two bundles that travel along the interventricular septum to excite the contraction of the ventricles.
Sinoatrial (SA) Node: Located in the right atrium, this acts as the heart’s natural pacemaker and initiates the heartbeat.
Atrial Spread: Excitation spreads across the walls of the right and left atria.
Atrioventricular (AV) Node: The electrical impulse reaches this node from the atria.
Bundle of His: From the AV node, excitation travels along the Bundle of His.